
Ths is a rejigged and updated version of an earlier article. Latest update 9/1/2021.

Covid-19 long haulers. Photo courtesy of LongCovidSOS.
Cognitive dysfunction and memory loss affect young Long Covid sufferers as much as those aged seventy and above, according to a new report by nine Covid long haulers from the United States and Britain.
Hannah Davis, who is one of the authors of the paper about the group’s patient-led research, tweeted: “One of the biggest findings to me was that there was no difference on age for the cognitive dysfunction, memory loss, or impact of these on daily life!! These happened as often in the 18-29 year old group as the 70+ group.”
In their paper, which was published on the preprint sever medRxiv on December 27, Davis et al. conclude that patients with Long Covid report prolonged problems in multiple organ systems, and significant disability.
“Most had not returned to previous levels of work by six months. Many patients are not recovered by seven months, and continue to experience significant symptom burden,” the researchers say.
Overall, they say, their findings suggest that the morbidity of Covid-19 illness has been greatly underestimated.
Davis, who is based in New York, tweeted: “The impact of Long COVID is substantial. 68% either required a reduced work schedule or were no longer working due to #LongCovid.
“For those with symptoms beyond 6 months, they continued to experience an average of 14 symptoms in month 7!”
The new paper reports on the results of an online survey and focuses on 3,762 long haulers from 56 countries who became ill between December 2019 and May this year. (People are defined as long haulers if they are sick for more than 28 days.) A total 91.6% of the survey respondents were not hospitalised.
The survey was open to individuals 18 years of age and older who experienced symptoms consistent with Covid-19, including those without positive SARS-CoV-2 diagnostic or antibody test results.
The resulting paper will be translated into more than ten languages.
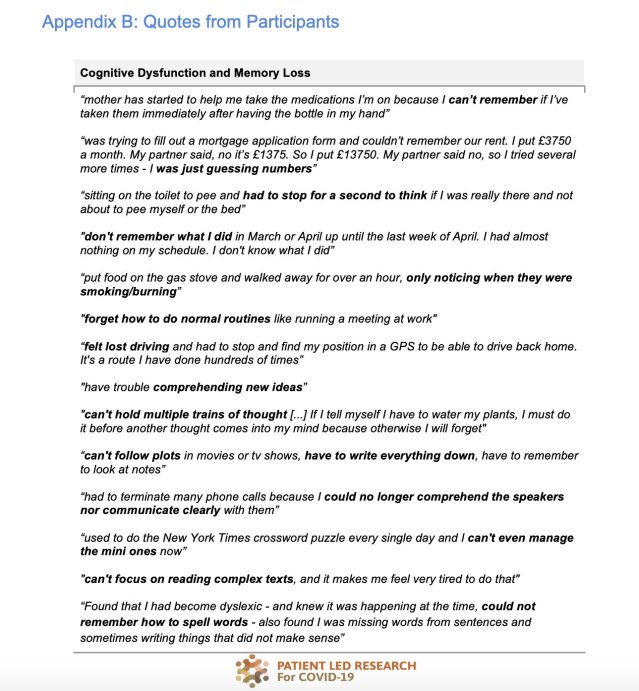
Davis et al. say that 88% of the 3,762 respondents experienced either cognitive dysfunction or memory loss.
“The greatest area of impact reported was on work, with 86.2% of working respondents feeling mildly to severely unable to work – 29.1% severely,” they write.
Participants reported having problems making serious decisions (85.3% of respondents), communicating thoughts and needs (74.8%), having conversations with others (68.3%), maintaining medication schedules (62.5%), following simple instructions (54.4%), and driving (53.2%).
“Memory symptoms, cognitive dysfunction, and the impact of these on daily life were experienced at the same frequency across all age groups,” Davis et al. say.
For 31.2% of survey respondents, the onset of brain fog/cognitive dysfunction occurred in their first week of symptoms.
Reports of cognitive dysfunction increased over the first three months, peaking at 66.7%, then decreased slightly in the following months. A total 55.5% of respondents experienced cognitive dysfunction during their seventh month of illness.
The most common symptoms were poor attention or concentration (74.8%), difficulty thinking (64.9%), difficulty with executive functioning (57.6%), difficulty problem solving or decision making (54.1% ), and slowed thoughts (49.1%).
Of the 72.8% of respondents who experienced memory impairments, 64.8% experienced short-term memory loss, 36.12% experienced long-term memory loss, 12.0% forgot how to do routine tasks, and 7.3% were unable to make new long-term memories.
Of those who experienced memory and/or cognitive dysfunction symptoms and had a brain magnetic resonance imaging (MRI) scan, 87% of the MRIs (345 of the 397 respondents who were tested) showed no abnormalities.
On May 11, a team from the Body Politic COVID-19 Support Group published a report resulting from 640 responses to a survey of patients suffering prolonged Covid-19 symptoms.
The main symptoms reported over eight weeks were shortness of breath, tightness in the chest, fatigue, chills or sweats, body aches, a dry cough, an elevated temperature (98.8–100), headaches, gastrointestinal issues, and brain fog.
About 91% of respondents said they hadn’t fully recovered. They had, on average, suffered symptoms for forty days.
The list of symptoms suffered by long haulers is lengthy. They range from extreme thirst, swollen lymph nodes, weight loss, hair loss, exhaustion, and joint pain to neurological problems such as numbness and muscle spasms.
People also suffer hallucinations and delusions, personality changes, panic attacks, dizziness, sensitivity to light and sound, eczema, blurred vision, stuttering, slurred speech, sleep disorders, and an increased heart rate.
Other problems include fevers that last for months, a poor sense of body movement and position, heat intolerance, difficulty standing, menstrual changes, tinnitus, persistent nausea, and newfound food sensitivities.
Loss of the sense of taste and/or smell is very common and the disorder that has become known as Covid toe (painful red or purple lesions) has been much publicised.
The nine long haulers who have published the most recent report say that, by the most conservative estimates, Long Covid currently affects 2.6 million people around the world.
The nine researchers work with several Long Covid support groups, including the Body Politic COVID-19 Support Group from which it originated. “Most of got sick in March 2020, before we knew anything about prolonged recoveries, and most of us are still sick nearly six months later,” they say.
The nine, who all have backgrounds in research and related fields, including neuroscience, public policy, data collection and analysis, and health activism, investigated the prevalence of 205 symptoms in different bodily systems and traced 66 symptoms over seven months.
They researched neuropsychiatric symptoms along with symptoms in the pulmonary, HEENT (head, ears, eyes, nose, and throat), gastrointestinal, cardiovascular, musculoskeletal, immunologic, dermatologic, and reproductive/genitourinary/endocrine systems. On average, nine of the systems were affected.
The most frequent symptoms reported after six months were: fatigue (77.7%), post-exertional malaise (72.2%), and cognitive dysfunction (55.4%). “These three symptoms were also the three most commonly reported overall,” Davis et al. say.
“In those who recovered in less than ninety days, the average number of symptoms peaked at week two, and in those who did not recover in ninety days, the average number of symptoms peaked at month two.”
Just 6.8% of the survey respondents recovered after day 28 of illness, and 93.2% were still experiencing symptoms at the time of survey completion.
Respondents with symptoms lasting more than six months experienced an average of 13.8 symptoms in the seventh month and 94.9% of respondents experienced relapses, with exercise, physical or mental activity, and stress as the main triggers.
Approximately half of the respondents indicated that their symptoms had slowly improved over time, 8.9% said their symptoms had gradually worsened, and 10.8% had symptoms that rapidly worsened over time.
Only 164 out of the respondents experienced a temporary break in symptoms. The remaining participants reported symptoms continuously, until symptom resolution or up to participating in the survey. A total of 2,454 respondents experienced symptoms for at least six months.
The researchers found that 86.7% of unrecovered respondents were experiencing fatigue at the time of the survey, 45.2% reported requiring a reduced work schedule compared with pre-illness, and 22.3% were not working at the time of the survey because of health problems.
Davis tweeted: “There are a few symptoms that seem to increase or happen in later months (months 6+) that more research/investigation is worth looking into: bone ache/burning, tinnitus, hearing loss, and other ear symptoms, and possibly eye/vision symptoms.”
Some respondents had fever for months, Davis et al. report.
Half of the reported symptoms were neuropsychiatric, the researchers found. Eighty-five percent of respondents reported cognitive dysfunction, about 91% suffered sensorimotor problems (tremors, tingling, and skin burning), 79% had sleeping issues, 77% had headaches, and 73% experienced memory loss.
Some serious symptoms are happening in #LongCovid: vision loss (1%), hearing loss (9%), new anaphalaxis (4%), new allergies (9%), facial paralysis (3%), suicidality (12%).
20% of respondents have changes in sensitivity to medications!! All doctors need to be aware of these. 16/
— Hannah Davis 🦈 (@ahandvanish) December 27, 2020
A total 86% of survey respondents reported experiencing cardiovascular symptoms. The most commonly reported symptoms were heart palpitations (67.4%), tachycardia (61.4%), and pain/burning in the chest (53.1%). A total 93% of respondents reported pulmonary and respiratory symptoms and 85.5% reported gastrointestinal symptoms.
Changes to taste and/or smell were reported by 57.6% of survey respondents. An altered sense of taste was experienced by 25.1%, phantom smells (i.e. olfactory hallucinations or phantosmia) by 23.2%, and an altered sense of smell by 19.8%.
The most common words used in describing phantom smells were smoke, burning, cigarette, and meat.
The most common hallucination reported was olfactory hallucination (23.2% of respondents). Visual hallucinations were reported by 10.4% of respondents, auditory hallucinations by 6.5%, and tactile hallucinations by 3.1%.
Some respondents reported post-menopausal bleeding or spotting and some women in their forties said they experienced early menopause. A total 26% of menstruating respondents reported having abnormal periods.
A total 15% of male respondents reported sexual dysfunction. There were reports of testicular pain and of a decrease in genital size.
Statistics office says one in five Britons are Covid long haulers
According to information gathered on the Covid Symptom Study app, which tracks sufferers regardless of whether they have had a test for SARS-CoV-2, about 300,000 people in Britain have reported symptoms lasting for more than a month, and 60,000 have been ill for more than three months.
The ZOE Covid Symptom Study, conducted in the UK and instigated by doctors and scientists working in partnership with the health science company ZOE, has produced figures suggesting that 12% of people in the country who contracted Covid-19 are still unwell after a month. One in 200 people said they had been suffering symptoms for more than 90 days.
Britain’s Office for National Statistics (ONS) says that about one in five people who test positive for SARS-CoV-2 exhibit Covid-19 symptoms for five weeks or longer and about one in ten exhibit symptoms for 12 weeks or longer.
The ONS has estimated that, during the week beginning on November 22, about 186,000 people in private households in England were living with Covid symptoms that had persisted for between five and 12 weeks.
The national statistics office says the data it released on December 16 was an “initial set of early experimental results”.
Among those with symptoms five weeks after testing positive for SARS-CoV-2 an estimated 11.5% of people were still experiencing fatigue, 11.4% had a cough, and 10% were suffering from headaches, the ONS says. Just over 8% were still experiencing a loss of taste, and 7.9% still had a loss of smell.
To conduct its analysis, the ONS researchers used Britain’s national Coronavirus (Covid-19) Infection Survey and linked healthcare and census datasets.
The ONS said: “Although this research is in its infancy, we felt it important to publish our early results in order to fill an important gap in the evidence base, and to provide a basis for discussion from which to inform the future direction of the research.
“This is our first attempt at producing these estimates, and the analysis is very much a work in progress. We will seek to further refine the estimates, for example by using more sophisticated statistical techniques to account for the possibility of relapse and, should sample sizes allow, investigate symptoms persisting beyond 12 weeks.”
Early next year, a new Long Covid question will be added to the Covid-19 infection survey. This will enable respondents to state the impact that Long Covid has had on their day-to-day activities and the question will include an expanded list of symptoms.
Th researchers also plan to utilise new Long Covid diagnosis information that is now being collected in computer systems used by general practitioners.
Long Covid sufferers welcomed the publication of the ONS results, but pointed to the limitations of the research and suggested how surveillance and analysis of Long Covid could be improved.
Nisreen Alwan, who is a medical doctor and associate professor from the Faculty of Medicine at the University of Southampton, noted in a thread on Twitter, that the denominator includes asymptomatic cases so the percentages of Long Covid among those who were initially symptomatic would be higher.
She said the list of symptoms used in the study was an ONS list that only referred to initial symptoms therefore some common Long Covid symptoms such as chest heaviness and pain, palpitations, and neurological symptoms are missing.
“Breakdown by age, sex, ethnicity, deprivation not available yet but will come hopefully,” Alwan tweeted.
“The importance of these estimates compared to other studies is the denominator of all those tested positive and the longitudinal nature of follow up rather than cross-sectional.”
In the ONS study, “recruitment” was not determined by the outcome (Long Covid) as it is in studies recruiting from support groups or clinics, which may give overestimates, Alwan noted.
“An even better way to #CountLongCovid is to follow-up everyone testing positive in the UK via Test & Trace and text them to ask if they’ve recovered or not by 5, 12 weeks & beyond,” she tweeted.
Alwan adds, however, that this doesn’t solve the problem of diagnosing people with Long Covid who have no positive test result for various reasons of availability, accessibility, timing and disincentives to testing. “For those we need standardised clinical case definitions, but we can base the probability of developing the condition on figures such as above,” she tweeted.
Elaine Maxwell, who is the author of a report about Long Covid that was published by Britain’s National Institute for Health Research (NIHR) in October, told The Independent that the ONS estimate could be lower than the reality.
She said: “The current ONS Covid-19 infection survey tracks a limited number of symptoms over time and may therefore not be capturing everyone with ongoing problems.
“The estimate of 186,000 people in England may prove to be an underestimate and the introduction of a wider list and the opportunity for people to describe the impact of Long Covid will hugely improve our understanding.”
Maxwell told The Independent that the ONS survey missed out vulnerable groups such as Travellers, the homeless, prisoners, and care home residents. “More work is needed to identify unmet need in these communities,” she said.
[UPDATE] In a report published in The Lancet on January 8, a team of Chinese researchers say 76% of patients they followed up had at least one Covid-19 symptom that persisted six months after they fell ill, and the percentage was higher among women than men.
“Lower antibodies against Covid-19 in patients six months after becoming ill compared with during acute infection raises concerns about the possibility of reinfection,” Chaolin Huang et al. added.
Follow-up tests on 94 patients after six months revealed that levels of neutralising antibodies were 52.5% lower than at the height of infection.
Chaolin Huang et al. studied 1,733 Covid-19 patients who were discharged from Jin Yin-tan Hospital in Wuhan between January 7 and May 29, 2020. The patients had a median age of 57 years. Follow-up visits were done from June 16 to September 3, 2020, and the median follow-up time was 186 days.
They found that, six months after acute infection, Covid-19 survivors were mainly troubled with fatigue or muscle weakness (63% of 1,655 patients), sleep difficulties (26% of 1,655 patients), and anxiety or depression (23% of 1,733 patients).
Patients who were more severely ill during their hospital stay had more severe impaired pulmonary diffusion capacities and abnormalities detected in chest imaging. They also performed less well in a test that measured the distance they were able to walk in six minutes.
More than 50% of the patients had residual chest imaging abnormalities, the researchers reported. Disease severity during the acute phase was independently associated with the extent of lung diffusion impairment at follow-up, with 56% (48 of 86) of patients requiring high-flow nasal cannula, non-invasive ventilation, and invasive mechanical ventilation during their hospital stay because of impaired pulmonary diffusion capacity.
Professor Bin Cao from the National Centre for Respiratory Medicine at the China-Japan Friendship Hospital, who is one of the report authors, said: “Because Covid-19 is such a new disease, we are only beginning to understand some of its long-term effects on patients’ health.
“Our analysis indicates that most patients continue to live with at least some of the effects of the virus after leaving hospital, and highlights a need for post-discharge care, particularly for those who experience severe infections.
“Our work also underscores the importance of conducting longer follow-up studies in larger populations in order to understand the full spectrum of effects that Covid-19 can have on people.”
The researchers say the full spectrum of post-discharge characteristics is still unknown and long-term follow-up studies on persistent symptoms, lung function, physical, and psychological problems of discharged Covid-19 patients are urgently required.
“Only a few studies with limited sample size have been published, with the longest follow-up duration of three months following discharge from hospital,” they said.
“No studies have yet reported the extra-pulmonary organ manifestations that could persist after damage in acute stage or are new onset after discharge.”
In a linked comment, Monica Cortinovis, Norberto Perico, and Giuseppe Remuzzi, from the Istituto di Ricerche Farmacologiche Mario Negri (IRCCS) in Italy, who were not involved in the study, wrote: “Unfortunately, few reports exist on the clinical picture of the aftermath of Covid-19. The study by Chaolin Huang and colleagues in The Lancet is relevant and timely.”
The study’s findings were consistent with those from earlier small studies that reported lingering radiological and pulmonary diffusion abnormalities in a sizeable proportion of Covid-19 patients up to three months after hospital discharge, Cortinovis et al. said.
“Evidence from previous coronavirus outbreaks suggests that some degree of lung damage could persist, as shown in patients who recovered from SARS, 38% of whom had reduced lung diffusion capacity 15 years after infection, they added.”
Unexpectedly, 13% of the patients who did not develop acute kidney injury during their hospital stay and presented with normal renal function, based on estimated glomerular filtration rate (eGFR) during the acute phase, exhibited a decline in eGFR at follow-up, Cortinovis et al. said.
“However, this finding must be interpreted with caution. Because repeated GFR measurement using a gold-standard technique … would presumably have been unfeasible in such a large cohort of patients,” they noted.
GFR-estimating equations, such as that used in Chaolin Huang et al.’s study, do not enable a sound assessment of renal function, which can be overestimated or underestimated compared with measured GFR, Cortinovis et al. added.
“Importantly, deep venous thrombosis was not diagnosed in any of the patients who underwent ultrasonography at follow-up,” they said.
“This is an encouraging finding, in light of the frequent development of venous thromboembolism in patients with Covid-19 who are critically ill while in hospital.”
All patients were interviewed face-to-face using questionnaires to evaluate their symptoms and health-related quality of life. They also underwent physical examinations, lab tests, and the six-minute walking test to gauge their endurance levels.
A total 390 patients had further tests, including an assessment of their lung function. [ENDS UPDATE]
Guidelines for managing Long Covid
On December 18 the National Institute for Health and Care Excellence (NICE) published guidelines for managing the long-term effects of Covid-19.
The guidelines cover care in all healthcare settings for adults, children, and young people who have new or ongoing symptoms four weeks or more after the start of acute Covid-19. The institute also makes recommendations about research.
The new guidelines include recommendations about identifying people with new or ongoing symptoms after acute Covid-19, the planning of care management, follow-up and monitoring, and continuity of care.
Seven members of the NHS Long Covid Taskforce and the Long Covid Support Group – Robin Gorna, Clare Rayner, Margaret O’Hara, Sophie Evans, Lisa Agyen, Natalie Rogers, and Claire Hastie – along with Will Nutland, who is an honorary assistant professor at the London School of Hygiene and Tropical Medicine, and Nathalie MacDermott, who is a member of the UK doctors’ Long Covid group (as is Clare Rayner), published a critique of the NICE guidelines in The Lancet entitled ‘Long Covid guidelines need to reflect lived experience’.
Gorna et al. say they have each lived with a range of symptoms lasting for more than six months.
“Staff in the UK National Health Service (NHS) have been variously supportive or disbelieving of our ongoing, often worsening, symptoms,” they write. “Before our illness we were fit, healthy, and working in demanding roles, including as doctors, nurses, and other health professionals.”
The nine say they are experiencing different patterns and varied severity of symptoms, but all share difficulties accessing adequate healthcare services. “Some of us have received misguided assessment and treatment in some of the UK’s recently established Long Covid clinics and encountered dismissive behaviour from some health professionals,” they write.
“Accurate assessment, diagnosis, treatment, and rehabilitation are especially important given the increasing evidence of organ pathology and impairment, with preliminary findings from 201 patients in a prospective, longitudinal, observational study suggesting up to 66% of people with Long Covid have organ damage and 25% have damage to multiple organs.”
Gorna et al. say guidelines should provide clear information on what is and is not known about the natural history of Long Covid, provide guidance for healthcare workers to identify cases, and inform clinical practice for the correct management of people with symptoms. The NICE guidelines do not do this sufficiently, they say.
The long haulers say the guidelines need to provide a more comprehensive description of the clinical features and physical nature of Long Covid. “Although the guideline notes that symptoms may fluctuate and often present as overlapping clusters, there is insufficient consideration of the apparent relapsing–remitting nature of the condition, which risks patients being discharged from clinics during a time of remittance of symptoms but before resolution of the condition,” they write.
They also say that the use of new nomenclature in the NICE guidelines, and notably the use of the term post-Covid-19 syndrome, is “rooted in unfounded assumptions about the pathology and not grounded in evidence”.
Gorna et al. say that guidelines must represent the complexity of Long Covid, including the areas where evidence is still emerging. “Hasty attempts to rename the condition or compare it to other conditions is a disservice to thousands of people, and could result in missed pathology to the detriment of the patient,” they write.
“Comprehensive Long Covid guidelines are essential to prevent an epidemic of long-term, chronic disease as a result of early mismanagement of pathology, and the potential implications of such an epidemic for health systems and economies.”
The authors of the critique say individualised rehabilitation plans are crucial – “not a one-model-fits-all approach”.
They say Long Covid healthcare services are also needed for children and young people. “There should be greater inclusion of people with Long Covid in clinical trials for potential Covid-19 treatments, including early interventions in the acute phase to prevent long-term complications, and there is a need for more long-term cohort studies of Long Covid,” they add.
“Additionally, a nationwide register should be established of people with Long Covid, and governments should report the data from this register with Covid-19 outcome data.”
The nine also propose that all clinics caring for people with persisting symptoms after acute Covid-19 provide a thorough physical assessment by a consultant physician from a medical specialty, “addressing first and foremost identification and management of any organ or multisystem dysfunction”.
Psychological aspects should be managed as part of the recovery process, but should not be seen as the primary treatment focus for all, Gorna et al. say.
Long hauler Barbara Melville-Jóhannesson tweeted: “I agree the new guidelines are welcome, and I share the concerns around timings and nomenclature. ‘Post-Covid-19 Syndrome’ will be used to abuse patients. We’ve seen this with other conditions.”

The report published by the Body Politic COVID-19 Support Group in May details the stark reduction in physical activity that occurs when people suffer from Long Covid.


One case referred to in the support group’s newsletter that was published on August 18 is that of Morgan, a group member who worked in tech prior to becoming ill.
After more than four months of illness, Morgan was still struggling with a host of debilitating neurological symptoms, including the inability to add simple numbers. “I’m incapable of sustained thinking, which for me means I’m incapable of working,” Morgan wrote.
“Demanding that my brain perform at this point could slow my recovery or leave me with limited capabilities. I have always been a knowledge worker, so thinking about that outcome is frightening.”
The newsletter’s authors state: “Long-term illness alters relationships, shrouds the future in uncertainty, and in too many cases, creates devastating economic hardship.”
They say support group members have been laid off or fired or have had to turn down job offers because of their myriad lingering symptoms.
“Some have resorted to working part-time, but worry about their ability to live off of this limited income for months or years to come. Many members, including healthcare workers, suspect that they contracted the virus while on the job. In quite a few of these cases, eligibility for workers comp is thwarted by false negative test results.”
On September 24, six women in Britain, including Nisreen Alwan, published an open letter drawing attention to the plight of Covid long haulers. The health problems faced by Long Covid sufferers needed to be addressed urgently, the women said.
The six women, who are all Covid long haulers, and are from diverse professional disciplines, said that the persistent symptoms following SARS-CoV-2 infection were now “one of the most pressing clinical and public health phenomena to address”.
They called for a “nuanced, patient-focused approach” – one that incorporates wide-ranging investigations of potential post-viral conditions and also recognises the pathogenesis of SARS-CoV-2 as specific in its own right.
“We need to avoid the severity or prevalence of ‘Long Covid’ being downplayed – whether for political purposes, privileging the claims that the economy is at odds with reducing levels of infection, or for fear of inadequately resourced healthcare systems,” Elisa Perego et al. wrote.
“We need to ensure the public knows about the potential ‘Long Covid’ consequences of infection when they are balancing the risks of exposure to SARS-CoV-2.”
The causes of Long Covid are unknown, the effects can be debilitating, and the percentage of patients affected is unclear, though likely significant, the letter’s authors said.
Doubts and imprecision about the meaning of the term Long Covid remain and an epidemiological definition is needed, they added.
The open letter, which was published on the Wellcome Open Research Platform and is entitled Why the Patient-Made Term ‘Long Covid’ is needed, was authored by Elisa Perego from the Institute of Archaeology at University College London; Felicity Callard from the School of Geographical and Earth Sciences at the University of Glasgow; Laurie Stras from the School of Music, Humanities and Media at the University of Huddersfield; Barbara Melville-Jóhannesson from the Creative Informatics department at the University of Edinburgh; Rachel Pope from the Archaeology, Classics and Egyptology department at the University of Liverpool; and Nisreen Alwan.
“We’ve tried here to bring together our expertise from the humanities, interpretive social sciences, arts, medicine and public health, science policy, patient involvement, and ethics in research,” the authors wrote.
Perego, Callard, Stras, Melville-Jóhannesson, Pope, and Alwan say that the personal, economic, and social costs of Long Covid are unfathomable and include screening; medical, rehabilitative and social care; and the costs associated with long-term disability, including lost productivity.
“Research indicating sequelae, even in asymptomatic/pauci-symptomatic cases, suggests screening and treatment may be needed for millions. The impact on already marginalised/minoritised communities will be particularly profound,” they add.
They say there is a need for greater specificity in measuring symptom duration, fluctuation, overall functionality, and quality of life as compared with pre-infection.
“Understanding ‘Long Covid’ is also crucial for prevention, and will help determine pandemic control policies,” they wrote.
Perego et al. say medical professionals, the media, and the wider community need to be sensitive to the trauma experienced by patients suffering from Long Covid.
“Some were left untended, to die at home; many were misunderstood or had their symptoms reduced to anxiety. Some have been caring for ill – or dying – family and friends, and many have lost jobs or are under threat of losing their livelihoods, medical insurance, or visa status.”
On August 24, Perego participated in a meeting with World Health Organisation officials that was called to address the challenges of long-term Covid-19 effects. About sixty long haulers from numerous countries, led by LongCovidSOS, a patient-led advocacy group in the UK, attended the online meeting.
Pauline Oustric from the French campaigning group #Apresj20 spoke about Long Covid support groups and campaigning initiatives that have emerged across Europe. She called for recognition, research, and rehabilitation, and for better communication about Long Covid. She urged the WHO and national governments to warn populations of the risks of Long Covid as a matter of urgency.
Hannah Davis was one of the long haulers who attended the meeting with the WHO. She told Brianna Sacks at BuzzFeed News that there were weeks when she couldn’t even remember how to send a text message.
“I feel like I have a brain injury,” Davis told BuzzFeed News. “I have a hard time remembering who I was. It was hard to remember I had to feed myself a couple times a day.”
Perego et al. say Long Covid is “a helpful and capacious term” that is needed to address the key medical, epidemiological, and socio-political challenges posed by diverse symptoms that persist beyond four weeks “after symptom onset that is suggestive of Covid-19”.
They add: “An international movement of patients (which includes all six authors) brought the persistence and heterogeneity of long-term symptoms to widespread visibility.
“The same grassroots movement introduced the term ‘Long Covid’ (and the cognate term ‘long-haulers’) to intervene in relation to widespread assumptions about disease severity and duration.”
The term Long Covid is now used in scientific literature, the media, and in interactions with the WHO, Perego et al. point out.
Perego et al. say that two other definitions, in addition to an epidemiological definition of Long Covid, need to be established: a “clinical case definition of Covid-19, which does not solely rely on laboratory confirmation”, and a “sophisticated definition for recovery that accounts for relapsing illness”.
Patient-led surveys made visible the diversity and persistence of Long Covid symptoms, Perego et al. say.
“Scientists do not yet know what causes long-term symptoms and incidence remains uncertain,” the women write. Case studies, they say, indicate that 10–87% of patients present persistent symptoms or fail to return to their health baseline three weeks after onset.
“These figures, however, derive from heterogeneous study designs and samples.”
There are vastly variable clinical manifestations of Long Covid, Perego et al. say.
“It may incorporate several conditions with different aetiologies and more than one mechanism, even in the same patient. Effects in multiple organs have been documented. On-going fatigue appears common.”
Perego et al. also say that, by deconstructing the current “mild-versus-severe” dichotomy, Long Covid “underlines that hospitalisation is an imperfect indicator of severity, even if has been used as such in studies”.
They add: “To rely on hospitalisation as a demarcation of severity creates skewed samples, including poor representation of younger/paediatric patients.
“In any case, persistent symptoms impairing an individual’s usual function and quality of life should not be called ‘mild’.”
Perego, Callard, Stras, Melville-Jóhannesson, Pope, and Alwan say that, while Long Covid patients have been provisionally defined as those who have not recovered within four weeks from symptom onset, “the point at which Covid-19 moves out of its acute phase remains unclear, and may vary in different patients”.
Duration and final outcomes of, and recovery from, Long Covid are also unclear, they say.
“Further research needs to address the complex host-pathogen interaction. While similarities between some ‘Long Covid’ symptoms and symptoms from conditions such as myalgic encephalomyelitis/chronic fatigue syndrome and dysautonomia need to be investigated, there is a risk of prematurely framing studies of ‘Long Covid’ through other diseases.
“This might downplay emerging phenomena specifically linked to Covid-19 – such as the range of SARS-CoV-2 action via ACE2 receptors widespread in the body, and the temporally and spatially complex immune response to the virus – thereby missing thresholds for early intervention.”
Lives turned upside down

Stephen Davis from PlanetEarth HD Documentaries tweeted six months after he contracted Covid-19 that he was suffering the symptoms of postural orthostatic tachycardia syndrome (POTS) along with skin flushing, headaches, tachycardia, and numbness.
Rachel Pope has tweeted about the severe pain in her heart and kidneys:

In an opinion piece published in the Los Angeles Times on July 9 David Lat, who is the founding editor of the legal news website Above the Law, talks about his “near-death experience with Covid-19”.
Lat spent 17 days in hospital, including six days on a ventilator. He had a lingering cough for two months.
“Recovering from a severe case of Covid-19 is not like switching a light on or off,” Lat wrote. “It’s more like a dimmer switch, where the light gets brighter, then darker, then brighter again …
“Before I came down with Covid-19, I could run for miles. After returning from the hospital, I needed a wheelchair to go even half a block.”
Lat wrote that he had improved dramatically since then, and many of his issues had resolved themselves.
“I graduated from the wheelchair to walking short distances to walking a few miles. My voice, hoarse because of how the ventilator damaged my vocal cords, slowly returned. I regained the 20 pounds I had lost (and then some). My cough, so forceful it made my chest and shoulders ache, finally went away. I can laugh again.
“But I’m still not back to normal, if normal means the way I was before Covid-19. I can’t jog – to say nothing of run – for more than a few minutes. I took a gallon of milk out of the refrigerator the other day for my son, and it felt like a 30-pound barbell. I tried reading a book about fire engines to him, and my voice, while much better than before, can’t make the “whoo-whoo” noise of a fire truck.”
The Atlantic’s science writer Ed Yong interviewed nine long haulers for an article published in June. One of them was Vonny LeClerc, a Glasgow-based journalist who told Yong that, on day 66 after she first started feeling shivery and flushed, she was still experiencing waves of symptoms.
“Before this, I was a fit, healthy 32-year-old,” LeClerc told Yong. “Now I’ve been reduced to not being able to stand up in the shower without feeling fatigued. I’ve tried going to the supermarket and I’m in bed for days afterwards. It’s like nothing I’ve ever experienced before.”
LeClerc said SARS-CoV-2 had ruined her life. “Even reading a book is challenging and exhausting. What small joys other people are experiencing in lockdown – yoga, bread baking – are beyond the realms of possibility for me,” she told Yong.
Alice Thomson wrote in an article published in The Sunday Times in Britain on September 23 that, six months after her Covid-19 symptoms started, she still can’t recognise smells.
“I still can’t tell the difference between the smell of an overripe banana or lavender. I can distinguish petrol but not gas, dog mess but not roses, bacon but not freshly cut grass. Everything else smells of burnt condensed milk,” she wrote.
Thomson still has her sense of taste, but feels slightly breathless when she goes for a run and finds that she bruises more easily than before.
“I have friends who haven’t been so lucky. We discuss symptoms and they vary wildly,” she wrote.
“Several have purple toes, two have hair loss another gets random rashes. A few have fared far worse. One friend, who’s 47, can still barely get out of bed 185 days after catching the virus; she has a constant high temperature, heart palpitations, body aches, chest pains, blue fingers and amnesia; at times she thinks she is going mad.
“A year ago we were running together in Hyde Park; now she can’t stir her soup. Her 75-year-old mother-in-law has moved in to nurse her and look after the children.”
Sandeep Lamba, from Gurgaon in India, is 26 and, before he contracted Covid-19, he was a competitive runner and played cricket and football. When Long Covid struck, his heart would race if he even tried to run and he is still unable to engage in sporting activities.
Lamba also suffered from severe anxiety, which hit mostly after 6 p.m., but could occur during the day and last for 24 hours or more, and he has been treated for weakness in a heart muscle, which his doctor said was caused by SARS-CoV-2 infection.
The anxiety, which began after Lamba was declared “recovered” (having had a negative PCR test), went on for nearly a month. His case of Covid-19, which was diagnosed on August 10, was mild and lasted two weeks. He says he has gone through a worse time as a long hauler than while he was SARS-CoV-2 positive.
Lamba says he still gets breathless sometimes, and experiences numbness on the left side of his body, mostly in his left hand and in his chest. He has weakened immunity because of Covid, so he easily becomes feverish or catches a cold.
Long hauler Talya Varga says she is seeking “rehab, research, and recognition” for those living with Long Covid.

In August, opera singer Lee David Bowen, aged 49, told Rhys Williams, reporting for the Caerphilly Observer in Wales, that he was still suffering the long-term effects of Covid-19 six months after first showing symptoms.
“I had a few days last week where I thought I was over it. It feels like you’re getting better, but then the symptoms come back. It’s crafty,” he said.
“My singing voice is in good shape thankfully, but I’m shattered after I practise,” Bowen told Williams.
Bowen told Williams he had been suffering “punishing fatigue”, a persistent metallic taste in his mouth, and brain fog.
“My mouth tastes like I’ve sucked a bag of two-pence pieces. I’m eating spicier foods to mask the bitter taste,” Bowen said.
Bowen told Williams that everyday tasks such as making breakfast, or just getting out of the shower, were exhausting.
Cherie Antoinette is a nurse, actress, writer, and film producer from Atlanta in the US who produces a blog called Eat Pray Nurse. She tweeted frequently during her time as a Covid patient, which was, on occasion, extremely traumatic, and continued to share her experiences during her recovery.
Antoinette suffered from insomnia and daily panic attacks. “I think it’s because my body remembers how scary nights were. Deep breathing has worked wonders. I’m trying to find a happy medium between relaxed and oversedated,” she tweeted.
Ironically, Cherie Antoinette said that she felt better during her recovery than she did before Covid. “Adding vitamins and drinking tea daily, decreasing my stress, and eliminating alcohol and caffeine have that effect.”
Although she was healthy, she says, she wasn’t taking care of her mental or spiritual well-being. “That’s not to diminish anyone else’s recovery from Covid. We all have our own journey. For me it was an eye-opening moment that I could do better,” she tweeted.
 Tim Spector (pictured left), who is a professor of genetic epidemiology at King’s College London, and is leading the Covid Symptoms Study said: “If you’ve got a persistent cough, hoarse voice, headache, diarrhoea, skipping meals, and shortness of breath in the first week, you are two to three times more likely to get longer term symptoms.”
Tim Spector (pictured left), who is a professor of genetic epidemiology at King’s College London, and is leading the Covid Symptoms Study said: “If you’ve got a persistent cough, hoarse voice, headache, diarrhoea, skipping meals, and shortness of breath in the first week, you are two to three times more likely to get longer term symptoms.”
He said that patterns in the data suggested that Long Covid was about twice as common in women as in men.
He added: “We do seem to be getting different symptom clusters in different ages, so it could be that there is a different type in younger people compared with the over 65s.”
Nick Peters, who is a professor of cardiology at Imperial College London and a consultant cardiologist, talked about responses to a questionnaire launched in March.
“Out of the 20,000 or so patients in total who have variously dipped in and out of the questionnaire about 3,000 report thinking that they have had Covid-19.”
Of the 3,000, about 1,600 patients gave information about symptom longevity. “Out of those 1,600 about 300 report symptoms lasting longer than two months,” Peters said.
 Nisreen Alwan, whose symptoms started on March 20, also participated in the webinar. She said that profound fatigue was a very common Long Covid symptom. The other symptoms she cites include coughing, breathlessness, muscle and body aches, heaviness in the chest, skin rashes, palpitations, fever, headache, diarrhoea, and pins and needles.
Nisreen Alwan, whose symptoms started on March 20, also participated in the webinar. She said that profound fatigue was a very common Long Covid symptom. The other symptoms she cites include coughing, breathlessness, muscle and body aches, heaviness in the chest, skin rashes, palpitations, fever, headache, diarrhoea, and pins and needles.
Alwan did feel better after several weeks and did go back to work full-time for a few weeks “then crashed again”.
She says that a very common feature is the fluctuating or relapsing nature of the illness. “You feel you’ve recovered … and then it hits you back, and it’s a constant cycle of disappointment, not just to you, but to the people around you.”
For months, Alwan said, she was struggling to open the freezer or load the dishwasher.
Alwan said that, as someone with Long Covid, “you learn your patterns, and you learn what actually brings on this utter exhaustion, and you learn what brings on the other symptoms as well, and you try and avoid these things”.
She added: “I’m fairly driven, and I thought I could beat this virus. A friend told me to stop dominating the virus and start accommodating it. Once you start accepting that, it becomes a bit easier. You have to drop your baseline by 90%; you are a different person.”
Alwan says Long Covid cases should be incorporated into Covid-19 statistics.
“By the end of June, so more than three months into me not going back to my normal health, I was very frustrated by the fact that no one was counting us,” she said.
“There was no quantification, no surveillance, of people who have not recovered from Covid.”
The experiences of thousands of people were not being validated and believed, Alwan said.
Alwan is one of a group of doctors who wrote ‘From doctors as patients: a manifesto for tackling persisting symptoms of covid-19’, which was published in the BMJ on September 15.
The doctors said that tackling Long Covid would involve collaboration between politicians, healthcare services, public health professionals, scientists, and society.
They called for action on four fronts:
- research and surveillance,
- clinical services,
- patient involvement, and
- access to services.
The doctors said that persisting Covid-19 symptoms should be dealt with using a scientific methodology, without bias. Services need to be timely, and tailored to individuals, “and involve investigating and treating pathology, as well as the functional recovery of individuals”, they say.
They also said that patients must be involved in the commissioning of clinical services and the design of research studies. Clinical services should not unfairly discriminate against those with negative tests and a clinical diagnosis should be adequate for accessing any appropriate services, they added.
“Adherence to positive test results as a criterion for access to medical services or specific Covid-19 sick pay arrangements with employers is unacceptable in the context of a clinical diagnosis of Covid-19,” the doctors said.

In an article published in the BMJ on July 21, Ingrid Torjesen reported on the advice given to doctors by the National Institute for Health and Care Excellence (NICE) that graded exercise therapy might not be appropriate for treating post-viral fatigue in patients recovering from Covid-19.
NICE noted that its previous advice on managing chronic fatigue might not be appropriate for patients recovering from Covid-19 and acknowledged that it could also be out of date for other groups, Torjesen reported.
NICE’s guideline on myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) was published in 2007, many years before the current pandemic, NICE said, “and it should not be assumed that the recommendations apply to people with fatigue following Covid-19”.
Torjesen says that he was “furious” when he read the 2007 NICE advice and the conclusions of the Cochrane review, which also supported exercise therapy and mentioned uncertainty about the side effects of adaptive pacing.
Group support
In an opinion piece published in the BMJ, four long haulers wrote about how a self-help pacing group has been helping them manage their Long Covid and has given them hope. The group, they say, is a safe space where they can talk about how they are doing and vent any frustrations.
The group members – Paul Garner, who is a professor of infectious diseases at the Liverpool School of Tropical Medicine and director of the Centre for Evidence Synthesis in Global Health; general practice trainee Iulia Hammond; trainee anaesthetist Linn Järte; and director of the Gingerhead branding and design agency Helen Calder – have been meeting weekly, online, for twenty minutes, and messaging each other when necessary.
The group, the long haulers say, has been a game changer. “Given the variety of our symptoms, we were all astounded that the management approaches that worked were so similar,” they wrote.
“We were all getting relapses; we jointly concluded that if we overdid it, these relapses were guaranteed, but the items of expenditure were different.”
Group members guide each other about how much exercise is advisable and how to get enough sleep.
“Managing pacing helps us prioritise our health,” the four wrote. “Two of us with children always put the children first, pushing through the fatigue. One runs her own business and needed to keep doing enough to protect her employees and not let down clients.
“Realising we had to be healthy to look after others assuaged the guilt of being less attentive to the children at home or placing heavier burdens on colleagues at work.”
The four long haulers all thought they were going to get better soon, but gradually became open to the probability that it might take much longer, perhaps twelve months.
“This was an important step and helped us make realistic goals, relieving the anxiety around the slow speed of recovery,” they wrote.
“All of us fear this illness might last for ever, but just saying it helps you feel better. We also witness each other improve, and are able to point this out, which gives a tremendous boost to our collective mood.
“As we learn to recover, we are not so lonely with our illness. We are healing, thanks to a little help from our friends.”
Statistics
According to the Centers for Disease Control (CDC) in the US, 35% of people who have been diagnosed with Covid-19 are not back to normal after “recovery”.
If the current recorded number of recovered Covid-19 patients in the US is correct (4.48 million), this would mean there are about 1.56 million long haulers in the US alone.
Researchers who carried out a study in Germany found that 78 out of 100 patients studied had heart complications two months after they were diagnosed with Covid-19.
Valentina O. Puntmann MD et al. said that cardiac magnetic resonance (CMR) imaging revealed “cardiac involvement” in 78 patients. The most prevalent abnormality was myocardial inflammation, which was detected in 60 people.
“These findings indicate the need for ongoing investigation of the long-term cardiovascular consequences of Covid-19,” they said.
They added: “Our findings demonstrate that participants with a relative paucity of preexisting cardiovascular condition and with mostly home-based recovery had frequent cardiac inflammatory involvement, which was similar to the hospitalised subgroup with regards to severity and extent.”
The median time gap between the patient testing positive for SARS-CoV-2 and undergoing the CMR examination was 71 days.
Puntmann et al. said that, on the day of the CMR examination, 17 patients reported atypical chest pain, twenty reported palpitations, and 36 reported ongoing shortness of breath and general exhaustion.
Twenty-five of the 36 said they were suffering symptoms during “less-than-ordinary daily activities”, such as household chores.
Italian researchers found that more than 87% of patients they studied, who had been hospitalised, still had numerous symptoms after two months.
In their study, Angelo Carfì and two other doctors from the geriatrics department at the Gemelli University Hospital in Rome found that, of the 143 patients studied, who ranged in age from 19 to 84 years, 87.4% reported persistence of at least one symptom, particularly fatigue and dyspnea (shortness of breath).
Patients were assessed for an average of two months after the onset of the first Covid-19 symptom. At the time of the evaluation, only 18 patients were completely free of symptoms related to Covid-19, 32% had one or two symptoms, and 55% had three or more. None of the patients had fever or any signs of acute illness.
Worsened quality of life was observed among 44.1% of patients, Carfì et al. say. A high proportion of people still reported fatigue (53.1%), dyspnea (43.4%), joint pain, (27.3%) and chest pain (21.7%).
The doctors said the limitations of the study included the lack of information on symptom history before acute Covid-19 illness and the lack of details about symptom severity.
“Furthermore, this is a single-centre study with a relatively small number of patients and without a control group of patients discharged for other reasons. Patients with community-acquired pneumonia can also have persistent symptoms, suggesting that these findings may not be exclusive to Covid-19,” they added.
Four clinicians working for the Assistance Publique–Hôpitaux de Paris in France published a paper in Clinical Microbiology and Infection on July 22, in which they report seeing an average of thirty long haulers (“patients for whom symptoms have not completely subsided”) every week from mid-May. Most of the women were aged about forty, and women outnumbered men four to one.
During a survey of more than 1,500 patients conducted by by Indiana University Medical School researcher Natalie Lambert and Survivor Corps¹, 98 different long-term symptoms were reported weeks and even months after infection with SARS-CoV-2.
Main survey findings
• The number of symptoms experienced by long haulers is much greater than that given on the CDC’s website.
• The survey results suggest that long haulers frequently experience neurological, eye, and skin symptoms.
• Survivor Corps group members frequently report reaching out to primary care doctors
for help with lesser-known and painful symptoms, but find that some physicians are unable or unwilling to help patients manage these symptoms because of a lack of research.
• A total 26.5% of symptoms experienced by long haulers were described as painful.


Source: July 25, Covid-19 Long-Hauler Symptoms Survey Report.

In a report about “post-Covid-19 fatigue, post/Long Covid-19 syndromes, and post-Covid myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)”, the honorary medical adviser to the ME Association, Charles Shepherd, writes that “as happens with ME/CFS”, there appears to be a significant female-to-male bias in people with Long Covid, but the bias is not as large as in the case of ME/CFS.
“Many are also previously fit young adults in their 20s, 30s and 40s,” Shepherd adds. “What is notable is the number who were regularly taking part in regular sporting activities, including running, and/or are health professionals.”
Perego et al. say that Long Covid may, mechanistically, include patients with symptoms variously deriving from direct viral damage, immune response damage, opportunistic bacterial infections, and post-viral/post-sepsis symptoms,
“Additional post-traumatic and mental health symptoms might interact with physiological symptoms in complex ways,” they write.
“‘Long Covid’ accounts for the possibility of persistent viral infection with low levels of viral shedding; protracted immune reaction; latency; or the presence of virus in reservoir organs or tissues.
“SARS-CoV-2 also appears to be able to reinfect, and to have the potential to precipitate new disease.”
Long Covid patients require prompt, multidimensional, diagnostic investigations and treatment – not least to rule out potentially life-threatening developments, Perego et al. say.
“Those who were not hospitalised, and those who were not tested or have negative PCR/antibody tests, must be able to access diagnostic and therapeutic services.”
Trauma and psychological symptoms are reported in both hospitalised and non-hospitalised survivors and need to be addressed sensitively, Perego et al. add.
“Differential diagnosis that does not reduce ‘Long Covid’ to psychological symptoms is crucial.”
The six women urge researchers and clinicians to tread a careful line that does not assume that symptoms are caused by anxiety; acknowledges that Covid-19 is frequently a traumatic experience; and considers many potential mechanisms in explaining mental health symptoms, including inflammatory responses and neurological damage.
Perego et al. also say there needs to be an adequate assessment of morbidity and mortality in ‘Long Covid’ cohorts, including in those who were not tested at the time of infection “or via effective serology screening, since testing is not exempt from pitfalls”.
Patients should be involved in the commissioning of research and clinical services, they add. “Many bring relevant expertise and some convene/own patient-led archives hosting extensive clinical data.”
There is potential for persistent illness to be caught up in political and medical misunderstandings and exploitation, Perego et al. say.
“The definition and treatment of complex phenomena (‘Long Covid’) that emerge in relation to an equally complex, currently not well understood disease (Covid-19), itself of contingent definition, are full of danger,” they write.
“We do not currently know whether all ‘Long Covid’ patients are indeed ‘post-viral’.
“While we acknowledge the importance of investigating comparisons with other diagnostic entities, we argue however against enfolding ‘Long Covid’ within other diagnoses.”
Perego et al. say there is a need for a label that is distinct from other phenomena related to earlier viral and other exposures, e.g. ME/CFS.
“We also question the term ‘Post-Covid Syndrome’. We believe it carries not only risks of misdiagnoses and mismanagement, but also of leaving those with persistent illness behind, especially in a post-vaccine world.”
There need to be collective responses to such questions as “Who will qualify for disability benefits/sick pay?” and “How will funds be allocated for research and treatment?” the six women say.
“Extensive involvement of ‘Long Covid’ patients has the best chance of ensuring that conceptualisation, investigation, and treatment of ‘Long Covid’ are attentive to the cultures, health systems, and discriminatory societies where patients live.
“‘Long Covid’ must not be understood as the outcome of biological processes alone.”


Measures to support Long Covid patients
On October 18 the National Health Service (NHS) in England announced a five-point package of measures to support Long Covid patients.
The chief executive of the NHS in England, Simon Stevens, announced that £10 million would be invested in helping to “kickstart and designate Long Covid clinics in every area across England”.
Stevens detailed the following measures:
- NHS England has asked NICE to issue new guidelines by the end of October about the “medical case definition” of Long Covid. This will include Covid-19 patients who have not been admitted to hospital or tested positive for SARS-CoV-2. NICE is then set to issue new evidence-based clinical guidelines in November about the support that Long Covid patients should receive. This will enable NHS doctors and other staff to provide clear, personalised treatment plans.
- An online rehabilitation service – ‘Your Covid Recovery’ – will provide personalised support to patients. The service, which was launched in July, gives people general information and advice about living with Long Covid. In Phase 2 of the project, patients will be able to access tailored rehabilitation plans.
- There will be designated Long Covid clinics where patients will be able to receive physical, cognitive, and psychological assessments and be referred to specialists when necessary.
- A team from the National Institute for Health Research will work with 10,000 Long Covid patients to better understand their condition and refine appropriate treatments.
- The NHS’s support services will be overseen by a new NHS England Long Covid task force, which will include Long Covid patients, medical specialists, and researchers.
Commenting about the issuing of new guidelines, the charity Patient Safety Learning said: “We welcome this measure and plans to update guidance so that it includes patients who may not have had a hospital admission or a previous positive test.
“We have heard from patients who have expressed their frustrations around the lack of clinical recognition of their illness, exacerbated by receiving a negative test result.”
The charity welcomed NHS England’s commitment to a one-stop approach to supporting Long Covid patients and said: “It is important that we recognise that patients may need to access a wide range of services and that patients who are unwell should not have to move between different clinical specialities to get diagnosis and treatment related to their personal needs.”
Patient Safety Learning said it appeared that the new measures would only be introduced in England. “We would be keen to clarify what steps are being put in place to support patients in the other three nations of the UK,” the charity said.
On October 15, Britain’s National Institute for Health Research (NIHR) published a comprehensive report about Long Covid in which evidence is drawn together that the author, Elaine Maxwell, says “demonstrates a significant and growing burden of need in a significant proportion of people who have are living with ongoing Covid-19”.
The NIHR says the ‘Living with Covid’ review draws on the most up-to-date expert consensus and published evidence, as well as the lived experience of both post-hospitalised and non-hospitalised Covid-19 patients “to better understand the impact of ongoing effects of Covid-19, how health and social care services should respond, and what future research questions might be”.
The institute adds: “There are powerful stories that ongoing Covid symptoms are experienced by people of all ages, and people from all backgrounds. We cannot assume that groups who are at low risk of life-threatening disease and death during acute infections are also at low risk of ongoing Covid.
“A working diagnosis recognised by healthcare services, employers and government agencies would facilitate patient access to much needed support and provide the basis for planning appropriate services. While it is too early to give a precise definition, guidance on reaching a working diagnosis and a code for clinical datasets is needed.”
The researchers found that the wide range of recurring symptoms experienced by both post-hospitalised and non-hospitalised Covid-19 patients affected the respiratory system, the brain, the cardiovascular system, the kidneys, the gut, the liver, and even the skin. The symptoms can range in intensity and duration and do not necessarily present in a linear or sequential manner.
Researchers found that Long Covid symptoms arise in one physiological system then abate only to arise in a different system.
They also report the following findings:
- There is a widespread perception that people either die, get admitted to hospital, or recover after two weeks, but it is increasingly clear that, for some people, there is a distinct pathway of ongoing effects.
- People experience a wide range of fluctuating and multisystem symptoms that need to be acknowledged.
- Ongoing Covid-19 needs to be considered holistically, both in service provision and in research.
- The varying degrees of dependency mean support in the community should be considered alongside hospital one-stop clinics.
- There are significant psychological and social impacts that will have long-term consequences for individuals and for society if not well managed.
- Health and social care services are not equipped to support people living with Covid-19. Staff need better information and education on the ongoing effects.
- There is an urgent need to better understand the symptom journey and provide realistic expectations about progression.
Maxwell says the following questions remain unanswered:
- What are the risk factors and who is at greatest risk of experiencing long-term problems?
- What is the impact of living with Covid-19 on families and carers?
- How can social support, including that provided by voluntary agencies, help?
- What are the financial pressures on previously economically active people?
- Acute Covid-19 infection has already had a disproportionate effect on certain parts of the population. Is this mirrored in ongoing Covid-19?
- Survivor Corps describes itself as “a grassroots movement connecting, educating and mobilising Covid-19 survivors with the medical, scientific, and academic research communities to help stem the tide of this pandemic and assist in the national recovery”.
There is a ‘Long Haul Covid-19 Symptom Compendium’ on this link.


DONATE TO CHANGING TIMES VIA SIMPLE PAYMENTS
1= 5 euro, x 2 = 10 euro, X 3 =15 euro, etc.
€5.00


 RSS - Posts
RSS - Posts










